
The Pilosebaceous Unit Through the Lens of MRBUP™
Moving Beyond Oil: Understanding the Living Architecture of Melanin-Rich Skin
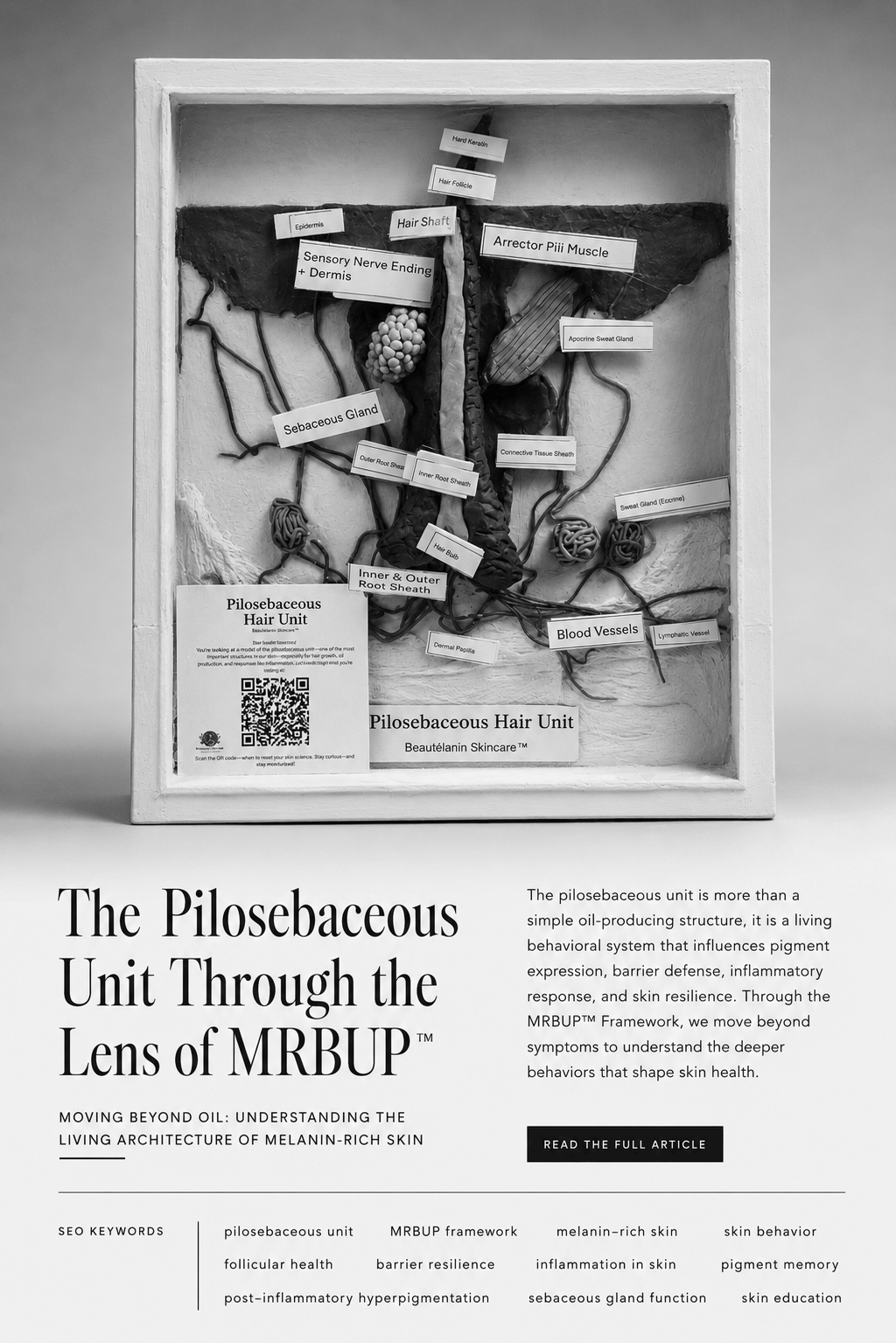
Pilosebaceous unit illustration showing the hair follicle, sebaceous gland, and sebum pathway
In traditional esthetics education, the pilosebaceous unit is often reduced to a simple explanation: a hair follicle attached to a sebaceous gland that produces oil. While technically correct, this definition fails to capture the complexity of the pilosebaceous unit, especially in melanin-rich skin. Traditional approaches tend to focus mainly on visible oiliness or blockages and often tailor treatment solely toward managing sebum production or superficial symptoms. In contrast, the MRBUP Framework invites practitioners to assess the pilosebaceous unit in terms of its deeper biological behaviors, such as barrier health, pigment activity, inflammation, and memory patterns—which allows for more targeted and effective treatment strategies tailored to each individual's unique skin behavior.
At Beautélanin™, we view the pilosebaceous unit as a dynamic biological communication center. It is not merely responsible for sebum production. It participates in barrier regulation, inflammatory signaling, pigment behavior, immune surveillance, thermoregulation, wound healing, and environmental adaptation. Through the lens of the MRBUP™ Framework, the pilosebaceous unit becomes one of the most important structures in understanding how skin behaves rather than simply how it appears.
The MRBUP™ Framework evaluates five interconnected dimensions of skin behavior:
M — Melanin Density
R — Reactivity and Inflammatory Response
B — Barrier Behavior and Resilience
U — UV Legacy and Pigment Activation
P — Pigment Memory and Pigment Mapping (aka Pattern Formation)
Each of these dimensions is directly influenced by the health and function of the pilosebaceous unit.
What Is the Pilosebaceous Unit?
The pilosebaceous unit consists of several interconnected structures:
* Hair follicle
* Hair shaft
* Sebaceous gland
* Arrector pili muscle
* Associated blood vessels
* Nerve endings
* Immune cells (Martel et al., 2024)
Together, these structures create a functional microenvironment that constantly responds to internal and external stimuli. (Al-Chaer et al., 2023, pp. 945-954)
The pilosebaceous unit serves as a gateway between the body’s internal systems and the outside world. Every day, it interprets signals from temperature, hormones, stress, UV exposure, microbial activity, friction, and inflammation. (Smith & Doe, 2015, pp. 123-130)
In many ways, the pilosebaceous unit functions as the skin’s environmental sensor network. When dysfunction occurs, the results may present as:
Acne
Hyperpigmentation
Folliculitis
Dryness
Excess oil production
Sensitivity
Delayed healing
Textural irregularities
However, these visible symptoms are often the consequence of deeper behavioral changes occurring within the pilosebaceous unit itself.
M — Melanin Density and Follicular Activity
Within the MRBUP™ Framework, melanin is viewed as an adaptive biological system rather than simply a pigment.
Melanocytes are present throughout the epidermis, but significant pigment activity also occurs within and around the hair follicle. The follicle serves as an important reservoir for melanocyte stem cells and pigment-producing cells. (Nishimura, 2011, pp. 401-410).This means that pigment behavior is often linked to follicular behavior.
When the pilosebaceous unit becomes inflamed or damaged, melanocytes surrounding the follicle may become overstimulated. This can trigger excessive melanin production and increase the likelihood of post-inflammatory hyperpigmentation (PIH). (Kaufman et al., 2018, pp. 489-503)
In melanin-rich skin, even minor follicular injury can activate a disproportionate pigment response. (Bakhsh et al., 2023)
This is why aggressive extractions, improper waxing, excessive exfoliation, and poorly selected treatments frequently leave dark marks long after the original injury has healed.
Under the MRBUP™ Framework, practitioners are encouraged to evaluate not only visible pigmentation but also the condition of the underlying follicular environment responsible for pigment activation. This assessment becomes practical when practitioners use specific cues to observe and question skin behavior around the follicle. Key observable signs may include: subtle darkening or shadowing around follicular openings, textural changes such as roughness or small bumps along the hairline or jawline, and areas where pigmentation consistently recurs after inflammation. In clinical practice, practitioners can further probe by gently asking clients whether certain areas tend to be more sensitive after procedures, if dark marks tend to reappear in the same spots, or if they notice lingering tenderness or itching in recently healed areas. Paying attention to patterns of follicular congestion, slight edema, or clusters of persistent pigment helps guide a more precise evaluation of the follicular environment.
R — Reactivity and Inflammatory Response
The pilosebaceous unit serves as one of the skin’s primary inflammatory response centers.
Every follicle contains immune cells, inflammatory mediators, blood vessels, and nerve connections capable of responding rapidly to perceived threats. (Mosca et al., 2025)
When irritation occurs, whether from heat, friction, harsh products, stress hormones, or microbial imbalance, the follicular unit often becomes one of the first structures to react.
Traditional assessments frequently focus on visible redness as a marker of inflammation.
However, many melanin-rich individuals do not display inflammation through obvious erythema. Instead, inflammation may present as:
Heat
Tenderness
Itching
Swelling
Follicular congestion
Pigment darkening
Delayed reactivity
The MRBUP™ Framework recognizes that inflammation is not always visible.
A client may demonstrate significant follicular inflammation while showing little to no visible redness. For this reason, practitioners must learn to assess inflammatory behavior rather than relying solely on visual cues. Non-visual indicators of inflammation can include increased local heat, tenderness upon palpation, subtle swelling, changes in texture such as roughness or bumpiness, and reports from clients of itching, sensitivity, or discomfort in affected areas. Incorporating light palpation, routinely asking clients about changes in sensation, and closely observing texture or pigment shifts can help practitioners detect inflammation early and support evidence-based practice.
The pilosebaceous unit often reveals these hidden inflammatory patterns before they become clinically obvious.
B — Barrier Behavior and Resilience
Sebaceous glands are essential contributors to barrier function.
The sebum produced by the pilosebaceous unit combines with sweat and epidermal lipids to form the skin’s protective acid mantle. (Brooks et al., 2024, pp. 509-521). When functioning properly, this system helps:
Reduce transepidermal water loss
Protect against environmental pollutants
Maintain microbial balance
Support wound healing
Preserve skin flexibility (Green et al., 2022)
Contrary to popular belief, oily skin does not necessarily indicate a healthy barrier. Many individuals experience simultaneous oiliness and barrier impairment. (Zhang et al., 2024, pp. 2109-2116)
In these cases, the pilosebaceous unit may increase sebum production as a compensatory response to dehydration or chronic irritation. (Mosca et al., 2025). This distinction is critical within the MRBUP™ Framework. Rather than asking whether skin is oily or dry, we ask:
How is the barrier behaving?
Is the pilosebaceous unit producing balanced protective lipids?
Or is it responding to dysfunction by overproducing oil?
Understanding this difference helps practitioners avoid treatments that further disrupt the barrier in an attempt to "control oil." Instead, the MRBUP Framework recommends a barrier-supportive approach focused on restoring balance and resilience to the skin. Practitioners can emphasize gentle cleansing with non-stripping formulas, recommend topical lipids or ceramide-rich moisturizers, support physiological hydration with humectants, and prioritize anti-inflammatory ingredients. Routine assessment of the barrier can guide the use of targeted treatments that respect the skin's natural defenses, helping to reduce excess oiliness while supporting overall skin health.
U — UV Legacy and Pigment Activation
The pilosebaceous unit also participates in the skin’s long-term response to ultraviolet radiation.
Hair follicles contain melanocyte stem cells that contribute to pigment production and repair processes following UV exposure. (Ferguson et al., 2015, pp. 1179-1189). Over time, repeated UV exposure creates what the MRBUP™ Framework refers to as UV Legacy.
UV Legacy reflects the cumulative biological memory left behind by years of environmental exposure. (Brenner et al., 2009, pp. 1002-1011). This history influences:
Pigment activation patterns
Inflammatory responses
Healing speed
Cellular resilience
Sensitivity thresholds
The follicular unit often stores evidence of these adaptive responses. As a result, two individuals with similar skin tones may respond very differently to identical treatments because their follicles carry different environmental histories.
The MRBUP™ Framework encourages practitioners to evaluate how UV exposure has shaped follicular behavior rather than relying solely on Fitzpatrick classification systems.
P — Pigment Memory and Pigment Mapping (aka Pattern Formation)
One of the most overlooked functions of the pilosebaceous unit is its role in pigment memory. Repeated inflammation around follicles can create recurring pigmentation patterns that appear remarkably predictable over time. (MPH & MMSc, 2024). Clients frequently report:
“I always get dark marks in the same place.”
“My acne heals, but the discoloration always comes back.”
“The pigmentation keeps returning in the same areas.”
These observations are often manifestations of pigment memory.
The follicular environment remembers previous inflammatory events.
Through repeated cycles of injury, healing, and melanin activation, the pilosebaceous unit develops recognizable behavioral patterns. (Daccache & Naik, 2024). The MRBUP™ Framework identifies these recurring patterns as evidence that the skin is responding according to its historical programming.
Rather than treating each dark spot as an isolated event, practitioners are encouraged to identify the underlying follicular behaviors responsible for recurring pigment activation.
The Pilosebaceous Unit as a Behavioral System
At Beautélanin™, we believe the pilosebaceous unit should not be viewed as a simple oil-producing structure.
It is a living behavioral system.
It responds to stress.
It remembers injury.
It adapts to environmental change.
It influences pigment expression.
It participates in barrier defense.
It communicates with the immune system.
Most importantly, it provides valuable insight into how skin behaves beneath the surface. When practitioners learn to interpret the pilosebaceous unit through the MRBUP™ Framework, they move beyond symptom management and begin recognizing the deeper biological patterns that shape skin health.
For example, consider a client who presented with recurring dark marks and breakouts along her jawline. Traditional assessment might have focused solely on controlling oil or lightening pigmentation. Using the MRBUP Framework, the practitioner noted subtle patterns: mild swelling after waxing, sensitivity on palpation, and repeated pigment clustering around certain follicles. Recognizing that these signs pointed to persistent barrier disruption and pigment memory, the treatment approach shifted. Instead of aggressive exfoliation, care focused on calming inflammation, supporting the skin barrier with gentle lipids, and adjusting hair-removal techniques to minimize follicular injury. Over several sessions, the client reported less tenderness, diminished breakouts, and a significant decrease in the recurrence of dark patches. This scenario demonstrates how MRBUP enables practitioners to identify and address underlying behaviors, leading to more lasting, individualized results.
The goal is no longer to fight oil, suppress pigment, or eliminate isolated symptoms.The goal becomes understanding the system's behavior. Because when we understand behavior, we can make better decisions. And when we make better decisions, we create conditions that allow the skin to function as it was designed to do.
References
Martel, J. L., Miao, J. H., Badri, T. & Fakoya, A. O. (2024). Anatomy, Hair Follicle. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK470321/
Al-Chaer, R. N., Bouazzi, D., Jemec, G. & Mogensen, M. (2023). Confocal microscopy and optical coherence tomography of inflammatory skin diseases in hairs and pilosebaceous units: A systematic review. Experimental Dermatology 32(7), pp. 945-954. https://doi.org/10.1111/exd.14830
Smith, J. & Doe, J. (2015). The Role of the Pilosebaceous Unit in Skin Homeostasis and Disease. Journal of Dermatology 45(3), pp. 123-130. https://doi.org/10.1016/j.jderm.2015.03.001
Nishimura, E. K. (2011). Melanocyte stem cells: a melanocyte reservoir in hair follicles for hair and skin pigmentation. Pigment Cell & Melanoma Research 24(3), pp. 401-410. https://doi.org/10.1111/j.1755-148X.2011.00855.x
Kaufman, B. P., Aman, T. & Alexis, A. F. (2018). Postinflammatory Hyperpigmentation: Epidemiology, Clinical Presentation, Pathogenesis and Treatment. American Journal of Clinical Dermatology 19(4), pp. 489-503. https://doi.org/10.1007/s40257-017-0333-6
Bakhsh, A. A., Alzubaidy, B. A., Attas, M. A., Miyajan, K. F. & Hawsawi, K. A. (2023). Follicular Variant of Acquired Dermal Macular Hyperpigmentation: A Case Report. Cureus 15(1). https://doi.org/10.7759/cureus.34133
Mosca, S., Ottaviani, M., Briganti, S., Nardo, A. D. & Flori, E. (2025). The Sebaceous Gland: A Key Player in the Balance Between Homeostasis and Inflammatory Skin Diseases. Cells 14(10). https://doi.org/10.3390/cells14100747
Brooks, S. G., Mahmoud, R. H., Lin, R. R., Fluhr, J. W. & Yosipovitch, G. (2024). The Skin Acid Mantle: An Update on Skin pH. Journal of Investigative Dermatology 145(3), pp. 509-521. https://doi.org/10.1016/j.jid.2024.07.009
Green, M., Kashetsky, N., Feschuk, A. & Maibach, H. I. (2022). Transepidermal water loss (TEWL): Environment and pollution—A systematic review. Skin Health Dis. 2022;2(2):e104. https://doi.org/10.1002/ski2.104
Zhang, X., Tao, H., Deng, Y., He, X., Zhang, Z., Zhong, L. & Wen, Y. (2024). Efficacy and safety of a panthenol-enriched mask for individuals with distinct impaired skin barrier subtypes. Journal of Cosmetic Dermatology 23(6), pp. 2109-2116. https://doi.org/10.1111/jocd.16231
Ferguson, B., Kunisada, T., Aoki, H., Handoko, H. Y. & Walker, G. J. (2015). Hair follicle melanocyte precursors are awoken by ultraviolet radiation via a cell extrinsic mechanism. Photochemical & Photobiological Sciences 14(6), pp. 1179-1189. https://doi.org/10.1039/c5pp00098j
Brenner, M., Coelho, S. G., Beer, J. Z., Miller, S. A., Wolber, R., Smuda, C. & Hearing, V. J. (2009). Long-Lasting Molecular Changes in Human Skin after Repetitive in situ UV Irradiation. Journal of Investigative Dermatology 129(4), pp. 1002-1011. https://doi.org/10.1038/jid.2008.325
MPH, S. D. & MMSc, J. F. (2024). Hyperpigmentation. Merck Manual Professional Edition. https://www.merckmanuals.com/professional/dermatologic-disorders/pigmentation-disorders/hyperpigmentation
Daccache, J. A. & Naik, S. (2024). Inflammatory Memory in Chronic Skin Disease. JID Innovations 4(3). https://doi.org/10.1016/j.xjidi.2024.100277
Beautélanin™ articles are for education only and do not replace medical advice.